Today, I bring to you a profile of my friend Ashley R. She does not blog, but she should. Ashley and I have been writing each for many many months online. I have used everything in my arsenal of knowledge to guide her, and she has been an excellent student. I take my role as Cushie advisor very seriously, and Ashley took my advice and made her own journey shorter as a result. I am very proud of her diligence and persistence, despite being very ill.
I finally met Ashley R. in Los Angeles this past January 2012. When she saw our shared doctor, Dr. Friedman, I drove her to the appointment.
Beyond what I have taught her, Ashley R. has been a wonderful teacher to me. She has become one of many Cushing's patients for whom I have deep admiration. Most importantly, Ashley R. and I have had many discussions, including how to enhance our outlook in order to create our new destiny without Cushing's and despite Cushing's. We are both committed to moving on to powerful and healthy lives that we have only because of the Cushing's. For this and many other reasons, I am proud to call Ashley R. my friend. I find her so compelling that I asked her permission to share her story here for you.
Ashley R. is having surgery in Houston at the MD Anderson Cancer Center on Friday, May 4 at 8 am. Please keep her in your thoughts and prayers.
"You have a brain
tumor? What the heck is Cushing's Disease?"
by Ashley R. on Thursday, May 3, 2012
at 4:20am ·
 I've spent
much of the last year being quiet about the changes in my body and mind. Yes,
there was chronic illness and debilitating/disfiguring symptoms, but I never
really wanted to take ownership of what was going on - it always seemed like an
invader to my body. I certainly didn't want to worry anyone unnecessarily and I
definitely didn't want to jeopardize any professional contacts by littering my
Facebook profile with too much medical information. For the most part, I tried
to keep as normal of a schedule as possible.
I've spent
much of the last year being quiet about the changes in my body and mind. Yes,
there was chronic illness and debilitating/disfiguring symptoms, but I never
really wanted to take ownership of what was going on - it always seemed like an
invader to my body. I certainly didn't want to worry anyone unnecessarily and I
definitely didn't want to jeopardize any professional contacts by littering my
Facebook profile with too much medical information. For the most part, I tried
to keep as normal of a schedule as possible.
... but I
knew things were changed. I knew that I couldn't keep up appearances for
long... so I (as gracefully as I could), withdrew from everything but what it
took to survive. If you were a part of my life that didn't make the cut, you
likely saw my involvement dwindle. I promise, I wasn't trying to hide. I was trying
to survive. I am fighting so I can come back to full involvement. I promise,
I'm almost there.
So here I
am, about a year and a half out from the initial start of this mess, and I am
ready to put pen to paper and explain what happened. Before I start, I need to
be laser clear on a few things:
1. I am so
grateful for the healing that this journey has brought to my life. This process
flipped my world upside down... and in the process, forced me to confront
things that I had avoided.
2. I am
confident that this is already cured and I am already healed ... my body is not
broken, and this was no mistake. I don't write this for sympathy -- I've
already grieved for what I thought I had lost. I write this story today from a
place of gratitude... gratitude for my friends and family who have supported me
through this and gratitude that I was trusted with this story. My prayer is
that I say what needs to be said and that there be no mistaking that Jesus has
been in control of the outcome from the beginning. I am at peace with what
happened.
Understanding
that, let's start at the present.
Today, I lay
in bed in a Houston hotel awaiting my turn to see one of the top neurosurgeons
in the country. Tomorrow, I will undergo brain surgery to remove a tumor from
my pituitary gland. Today, I pray, is the last day Cushing's Disease is allowed
to be in my body.
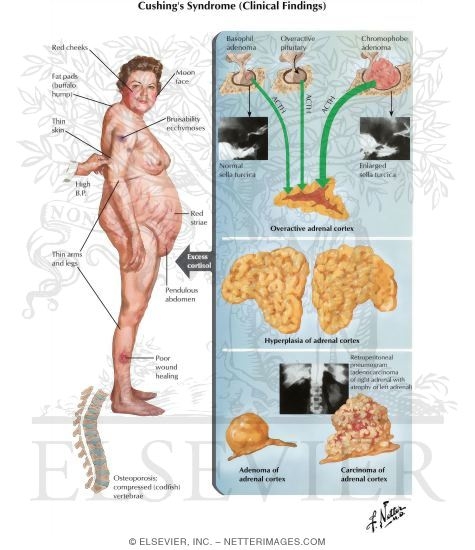
What is
Cushing's Disease?
Ever heard
of the stress hormone, cortisol? Cushing's Disease is simply (ha!) an
overproduction of cortisol in the body, usually caused by a tumor that overproduces
the "give us more cortisol" hormone (ACTH).
Picture for
a moment a time in your life when you experienced EXTREME STRESS. Perhaps you
went through a trauma of some kind...perhaps you had a point in time where you
had too much "critical" stuff to do and not enough time. Picture how
your body felt - your muscles twitching between super strong and super goo,
your heart beating fast, your head going from clear to mush... your appetite
dropping only to hours later leave you ravenous... your body switching to
survival mode with only one objective: run away from the tiger before it eats
you.
Got it?
Now picture
never being able to shut that off.
That, is the
only way I can give you a glimpse of what this disease process looks like.
Take a few
moments and watch this video -
it explains the technical side of things quite well. It is worth the 6 minutes.
How did it
happen to me?
I'm not
really sure... but as I looked over the patterns in my life, it is entirely
possible this is something I've been cycling with since I was a young girl. We
started to get suspicious January 2011 when an overwhelming amount of fatigue
took over my body and I gained about 30 pounds in 30 days - while dieting,
walking 3 miles a day, and regularly practicing EFT to work through the
emotional side of things. Something was wrong, something was very, very wrong.
As I
scrambled for answers (surely, I had to be doing something wrong), a friend
mentioned Cushing's. I scoffed, "now why would I want that? That's not
fun."
A few weeks
later, Samuel picked me up in San Luis Obispo and drove me to Seattle to be
seen and have initial tests run. When the tests came back showing that we were
on the right path, the choice was made immediately to move me back to Seattle
permanently.
I didn't
struggle through doctor after doctor who told me I was crazy. I didn't have the
energy for that... I went straight to one of the leading experts on Cushing's
Disease. For 8 months, I tested - blood draws, 24 hour urine collections, and
saliva tests... Over and over again. Trip after trip to the lab. It was an
exhausting and humiliating experience. Scratch that... it was an exhausting and
humbling experience.
I tried to
stop the process. I tried hard to fight it. When I stopped fighting it, there
was a bit of a lull to the process. It made no sense. Throw everything you know
about your body out the window. I was gaining weight eating a clean paleo diet
and could get the weight gain to stop if I ate crap junk food. It made no
sense. None. It still doesn't.
By
September, most of the changes in my body had already occurred. I had gained
about 150 pounds in a little over 7 months. My waist circumference doubled. My
hair fell out. Reddish purple lines striped my arms, shoulders, and chest. Pads
of fat seemed to grow both at the back of my neck AND on top of my collarbone.
My face COMPLETELY changed. My moods altered and I fought against rage in my
body. My skin turned both bright red and orange. Anxiety and paranoia were
present daily.
While I've
avoided posting pictures over the last year, I feel like none of these words
can quite show the change like this photo can. This my friends, is what the diagnostic
process cost me physically.
 |
| end of December 2010 ------------------------- April 2012 |
Dramatic,
eh? It was only 16 months.
I've tried
(sometimes unsuccessfully) to rationally think through these changes. I've
tried to keep perspective - that most of these things I felt were caused by the
hormones NOT by real threats. In short: I did everything I could to not BLAME
this disease process for any of my shortcomings. There were definitely
limitations, but I refuse to give in completely and let this disease process
take more than it needed to.
We found the
tumor in October via MRI. You'd think, with an ever growing mountain of
evidence supporting a diagnosis AND a visible tumor, that the doctors would be
clamoring to take that puppy out, right? That just wasn't the case.
Midway
through November 2011, I learned that my doctor was retiring his practice and moving
in to drug research. I never managed an official diagnosis out of him -- the
day he left his practice, he had spent 8 months being "highly
suspicious" but never committal. Is this a doctor thing or a man
thing? Who knows.
 |
| my buffalo hump |
In January 2012,
I flew to California to see another Cushing's specialist. There were several of
you who prayed for and helped fund this trip. I am eternally grateful for your
generosity.
When I met
one of the doctors the first thing he said to me was, "Why hasn't anyone
helped you before now? Why did they let you get this sick?" I do not have
an answer to that question.
I spent most
of February and the early part of March doing one final blitz of testing. In
truth, the doctor likely had enough to make the final call, but needed tests
that he had ordered to come back positive to do the whole CYA thing.
Mid March 2012,
almost a year to the day of my first appointment to discuss Cushing's Disease, I
had a diagnosis: Cyclical Pituitary Cushing's Disease.
Over the
year and a half of progressively getting sicker, I was asked many times why I
fought so hard for a particular diagnosis. After all, most people are
traumatized when they hear they have a tumor and a life threatening illness. I,
on the other hand was relieved.
I have a
short answer to this: I needed 100% written proof, verified by a professional,
that I did not intentionally do this to myself. I needed that proof for me...
and for anyone else that would raise an eyebrow to me.
Sound
strange? Sound selfish? Sound a bit ridiculous? Probably.
You see, I
grew up an overweight child. I was blamed, from the age of...oh...8 or 9... for
my weight problems. I've had so many labels put on me by doctors that refused
to look for something other than a sad child who liked chocolate. I needed the
diagnosis because I spent decades hating those responsible for my physical and
emotional well being. I couldn't put my finger on it... but I never bought what
they were saying.
The
Cushing's diagnosis gave me the courage to forgive.
The process
to get the diagnosis gave me the ability to appreciate and love my body in a
way I can't quite explain - though I am going to try later this week.
Anyway,
here's what's next:
I'll have
drive by brain surgery through my nose on Friday... then we pray that it is a
cure. The surgery is really easy guys - I promise I am going to be ok... I am
at one of the best facilities in the world and have one of the top surgeons in
the world. He knows this disease inside and out and is going to take good care
of me. Yes, please pray for me and for him for the actual surgery... but also
keep my family in your prayers... as they are the ones who have to anxiously
await the good news. Dad, Kelly, and Sam are here with me... and my sister is
back up in WA (worrying no doubt).
Once I
return home, I get a new fight on my hands: the "drying out" process
(allowing the cortisol soaked tissues to get rid of the excess stored cortisol)
and the "waking up" process (where my body starts producing hormones
on its own again). They say the cortisol withdrawal is akin to a heroin addict
going through withdrawals. Please pray for me. Please come check on me. This
process scares me more than anything else.
Then, we
rebuild from a place of gratitude. We learn from the process... and we move
forward.
I am
overwhelmed by the support, prayers, and generosity of those around me. I am
overwhelmed at the humility my husband has shown through the whole process (I
love you!). I am overwhelmed by the support of my bosses and coworkers - I've
never felt more cared about by any other group of women. I am overwhelmed that
women I didn't know came to visit me when I first moved back to Seattle and was
lonely because no one was coming to see me. I am overwhelmed by the knowledge
I've had the privilege of acquiring. I'm overwhelmed by the courage of the
women who have gone before me in this fight - the women who took their time to
navigate this process and support me every step of the way. I am overwhelmed
that you took the time to read this... and mostly, I am overwhelmed that Jesus
has been there through it all, going ahead of me, carrying me, and providing
what I needed to come out on the other side of this in a much better place than
when I went in.
Thank you so
much for everything you've done and for the love you've shown to me.
All my love,
Ashley R.







{kind=link}