
Thursday, February 20, 2014
Tuesday, February 18, 2014
Cushing's Changes You

Monday, February 17, 2014
Happy Presidents Day!
Today, I share a special Presidents Day treat. It brings a smile to my face to know what is possible for me.
BLAers and pre-BLAers.
We can manage our daily stress. If JFK could do it running campaigns and being president, we can manage our family and lives. Kid's science fair project/ birthday party or Bay of Pigs/ Cuban missile crisis? "The only thing to fear itself."
http://www.nytimes.com/2002/11/17/us/in-jfk-file-hidden-illness-pain-and-pills.html
Here is another post I made about JFK's frail health in June 2009:
http://cushingsmoxie.blogspot.com/2009/06/jfk-had-adrenal-trouble-too.html?m=1
and November 2013
http://cushingsmoxie.blogspot.com/2013/11/character-above-all-john-f-kennedy.html?m=1

Friday, February 14, 2014
You are the Medical Expert
I hear this question among Cushies and non Cushies alike:
Should we change our cortisol dose on our own or wait to speak to a doctor first?
This is my very strong and firm opinion, as a Cushie/Addie who had lived with a type 1 diabetic.
Make no mistake.
A doctor would NEVER tell a diabetic to call them in a low or high and NOT adjust his/her insulin dose without talking to the doc or nurse first. A diabetic would die waiting for a doc's reply. A BLAer could, too.
BLAers, you must adjust your dose as needed. We have no cortisol meter like diabetics have glucometers. We must trust ourselves. We must trust our bodies and symptoms that tell a story. We must base every decision regarding cortisol dose on how we feel and compare/contrast that to what other BLAers feel. Then make the decisions for ourselves.
Doctors are there to check in with regularly, to order tests, to give us a big picture perspective. The collective knowledge that this group of 83 Cushies has is greater than 99% of the doctors who give us instructions. They have never done it! They will give us the textbook version that, in reality, has taken years to write, edit and publish. A Cushie's knowledge is current, fresh and open to new ideas. We all want to feel better and we will fight to get better.
Do what you can to be your own medical expert. The truth, you are already.
Thursday, February 13, 2014
National Organization of Rare Diseases Supports Cushies with Grants for Medical Expenses
APPLY NOW:
NORD ANNOUNCES NEW CUSHING'S SYNDROME PATIENT ASSISTANCE PROGRAM
In partnership with Corcept Therapeutics Inc., the National Organization for Rare Disorders (NORD) has established a Cushing's Syndrome Patient Assistance Program for patients with endogenous Cushing's syndrome who need financial assistance with certain costs related to their medical diagnosis and/or care.
Endogenous Cushing's syndrome is a serious and debilitating rare disorder caused by over-production of cortisol, a steroid hormone that increases blood sugar levels, by the adrenal glands. The syndrome most commonly affects adults between the ages of 25 and 40.
"It is especially appropriate that we are making this announcement just before Cushing's Awareness Day, which will be observed on Sunday," noted NORD President and CEO Peter L. Saltonstall. "The Cushing's Support and Research Foundation (CSRF), a non-profit organization for patients and families affected by Cushing's syndrome, is a member of NORD. We are pleasd to join CSRF and the entire Cushing's community in promoting awareness of Cushing's syndrome at this time."
The new program, which launches on April 11, will provide assistance with deductible and/or co-pay expenses to ensure patient access to Korlym, a drug developed by Corcept and approved by the Food and Drug Administration earlier this year.
The program will also provide financial assistance to eligible uninsured and underinsured patients for reasonable expenses required for diagnosis, direct treatment, and care that are not covered by insurance. These would include incidental medical expenses such as lab and diagnostic tests, as well as related expenses such as travel for a medical consultation.
Patients seeking information about the program, or to apply, may contact NORD through a toll free phone number (800 999-6673 Ext. 326) or by email (cushings@rarediseases.org).
Prior to FDA's approval of Korlym on Feb. 17, 2012, there were no approved medical therapies for the treatment of endogenous Cushing's syndrome. Korlym is approved for use in patients with endogenous Cushing's syndrome who have type 2 diabetes or glucose intolerance and are not candidates for surgery or have not responded to prior surgery.
NORD is a nonprofit organization, established in 1983, that represents the 30 million Americans with rare diseases. In addition to patient assistance programs, NORD provides programs of advocacy, education, awareness, and research.
There are other programs that NORD lists on its webpage here:
http://www.rarediseases.org/patients-and-families/patient-assistance
http://www.rarediseases.org/patients-and-families/patient-assistance
Saturday, February 8, 2014
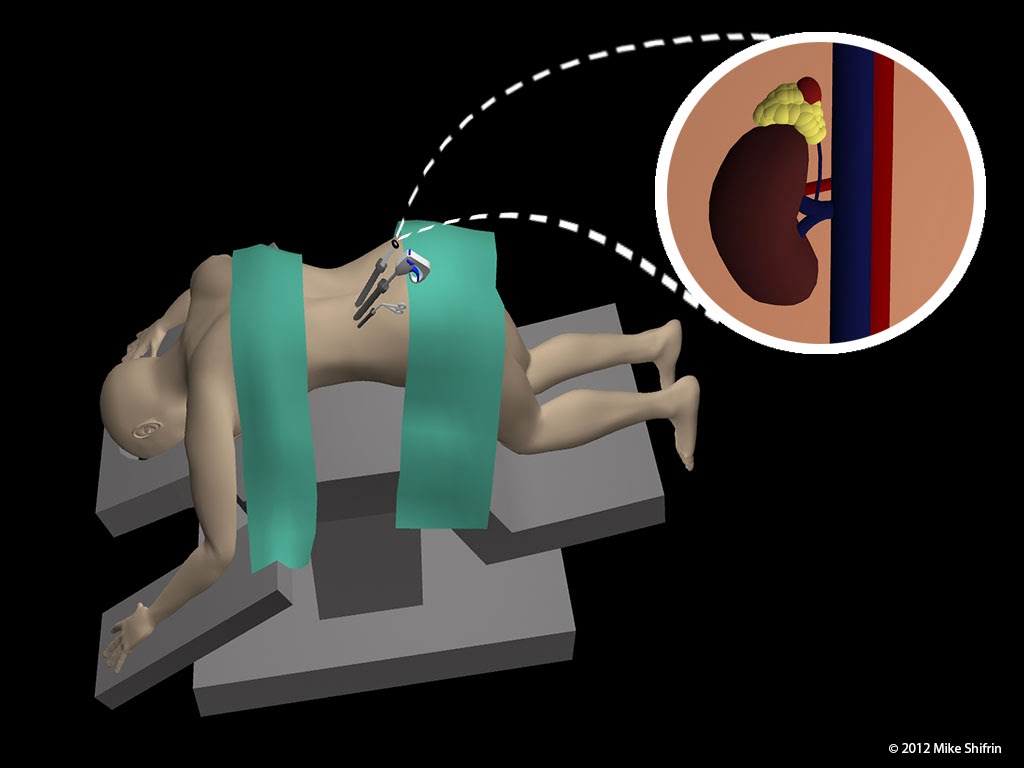
Laparoscopic Right Adrenalectomy

http://emedicine.medscape.com/article/1894961-overview
Thursday, February 6, 2014
Empower EMS nationwide to administer the life saving drug solucortef in emergencies for Adrenal Insufficient patients. | We the People: Your Voice in Our Government
EMS must be required to carry Solu-Cortef of ambulances. We are currently fighting state by state to get this basic protection in place.
Two years ago, I wrote the following post. Now, I'm face adrenal insufficiency every day.
http://cushingsmoxie.blogspot.com/2011/12/my-friends-with-adrenal-insufficiency.html?m=1
This White House petition has 771 signatures when I received this right now. Let's add to the list, Cushies!!! The life you save may be your own.
https://petitions.whitehouse.gov/petition/empower-ems-nationwide-administer-life-saving-drug-solucortef-emergencies-adrenal-insufficient/NvTT0h6b
Two years ago, I wrote the following post. Now, I'm face adrenal insufficiency every day.
http://cushingsmoxie.blogspot.com/2011/12/my-friends-with-adrenal-insufficiency.html?m=1
This White House petition has 771 signatures when I received this right now. Let's add to the list, Cushies!!! The life you save may be your own.
https://petitions.whitehouse.gov/petition/empower-ems-nationwide-administer-life-saving-drug-solucortef-emergencies-adrenal-insufficient/NvTT0h6b
Solu-Cortef administration

Someone forwarded this to me.
Finally. Simple to use instructions.
Trouble refilling Solu-Cortef
I tried to refill my prescription of Solu Cortef. The Pharm Tech told me they no longer have this Rx. I knew about the new number but I forgot it and had to find it. Good thing my blog serves as my own persona filing cabinet.
Please remember to notify your pharmacy of the change to the drug number so it can be found in their system. Or, remember you can search for my blog and Solu-cortef and find it. This is super important. It's life-saving medication.
http://cushingsmoxie.blogspot.com/2012/04/day-23-file-it-awaysolu-cortef-has-new.html?m=1
Please remember to notify your pharmacy of the change to the drug number so it can be found in their system. Or, remember you can search for my blog and Solu-cortef and find it. This is super important. It's life-saving medication.
http://cushingsmoxie.blogspot.com/2012/04/day-23-file-it-awaysolu-cortef-has-new.html?m=1
Cortisol pumps in the future
I hope BLA patients will be next to be included in the study. We can benefit from a pump just as type 1 diabetics do. Right now, we BLAers are like diabetics without meters. So much progress can be made in this realm of cortisol replacement and administration.
http://www.magicfoundation.org/www/docs/100.2950
http://www.magicfoundation.org/www/docs/100.2950
Thursday, January 30, 2014
Difficult to Diagnose
Almost seven years after I first was dismissed over my concerns I suffered from Cushing's, I am disheartened to talk with undiagnosed Cushies who are suffering the same way.
There is just no good reason. That's right I said it. THERE IS NO GOOD REASON THAT CUSHIES AEE SUFFERING TO GET DIAGNOSED AND TREATED.
Always in an effort to put these dots close together for our medical professionals, I am posting a Moxie favorite. This lists the most common symptoms of Cushing's. Print it and fill it out. Add other symptoms.
If your doctor dismisses you, don't get too discouraged. Dismiss her/him! On the spot! Please don't allow anyone to ignore and silence you. Like bad boyfriends and bad girlfriends, don't waste one more minute on a bad relationship.
You are a bright shining star, and when you get better, you will shine bright again. Get yourself there.
http://www.korlym.com/docs/KorlymSymptomsChecklist.pdf
There is just no good reason. That's right I said it. THERE IS NO GOOD REASON THAT CUSHIES AEE SUFFERING TO GET DIAGNOSED AND TREATED.
Always in an effort to put these dots close together for our medical professionals, I am posting a Moxie favorite. This lists the most common symptoms of Cushing's. Print it and fill it out. Add other symptoms.
If your doctor dismisses you, don't get too discouraged. Dismiss her/him! On the spot! Please don't allow anyone to ignore and silence you. Like bad boyfriends and bad girlfriends, don't waste one more minute on a bad relationship.
You are a bright shining star, and when you get better, you will shine bright again. Get yourself there.
http://www.korlym.com/docs/KorlymSymptomsChecklist.pdf
Wednesday, January 29, 2014
No "Minor Surgery" after BLA
There is no such thing as a minor surgery or a simple outpatient procedure. This is one if many ways that life without adrenals changes. A normal body uses cortisol to cope with the trauma that occurs to the body during these "easy" procedures.
Before you have dental or medical procedure, please understand how to increase your steroid coverage to keep yourself out of adrenal crisis.
Follow this link to very detailed information outlining how much steroid to take for different procedures and operations.
http://www.addisons.org.uk/comms/publications/surgicalguidelines-colour.pdf
Aldosterone can be just as important as Cortisol

Our good friends at Stop the Thyroid Madness shared this post about aldosterone. For a recent BLAer, this importance of this hormone cannot be overstated. Cushies are adjusting cortef/hydrocortisone doses and fludrocortisone doses. The scary part is that many of us feel lost and quite get a grip on this hormone and what it means and how to adjust based on our lab results. Well, here is some information I'm slot trying to commit to memory. My Cushie brain is still dull and unable to learn new material.
Aldosterone can be just as important as Cortisol
http://www.stopthethyroidmadness.com/aldosterone/
"Low cortisol due to worn out adrenals is common among a large body of hypothyroid patients, and it can be necessary to supplement with cortisol, or bring it up with the T3CM. But along with cortisol, there's another adrenal hormone that you may need to investigate with your doctor: aldosterone.
Much more about this in the revised STTM book here.
WHAT IS ALDOSTERONE? Aldosterone, a steroid hormone just like cortisol, is produced in the outer cortex of your Adrenals (along with cortisol, testosterone, DHEA, DHEAS, androstenedione and estrogens). Aldosterone is the principal of a group calledmineralocorticoids, and it helps regulate levels of sodium and potassium in your body–i.e. it helps you retain needed salt, which in turn helps control your blood pressure, the distribution of fluids in the body, and the balance of electrolytes in your blood. It does all this by stimulating your kidneys to both take in more sodium while releasing excess potassium–a vital balance in your heath and well-being.
WHAT EXACTLY STIMULATES ALDOSTERONE PRODUCTION? Several things will stimulate your aldosterone secretion: when you potassium levels go too high, if there is less blood flow to your kidneys, or if your blood pressure falls. On the other side of the coin, aldosterone secretion will falls if your potassium levels fall, the blood flow in your kidneys increases, blood volume increases…or if you consume too much salt.
WHAT HAPPENS IF ALDOSTERONE GETS TOO HIGH OR LOW? When aldosterone gets too high (as it can under stress and as your cortisol goes too high), your blood pressure also gets too high and your potassium levels become too low. You can have muscle cramps, muscle weakness, and numbness or tingling in your extremities.
But when it gets too low, which can be common in some patients with cortisol deficiency, your kidneys will excrete too much salt, and it leads to low blood pressure; low blood volume; a high pulse and/or palpitations, dizziness and or lightheadedness when you stand; fatigue; a craving for salt. Symptoms of low aldosterone can also include frequent urination, sweating, a slightly higher body temperature, and a feeling of thirst, besides the craving of salt. Potassium can at first rise too high, then fall, as well.
A CLUE: Is your dog licking your legs? That is indicative of the salt wasting by low aldosterone.
Another clue that your aldosterone may be too low is being on high amounts of HC, such as 30-40 mg, and not getting good results…i.e. you seem to be continually chasing stable temps. (Before getting on HC, learn of a way to raise low cortisol with the T3CM.)
WHAT ROLE DOES ADDING SEA SALT AS A SUPPLEMENT PLAY? Adding salt, but specifically sea salt, can be beneficial to treat the symptoms of low aldosterone. Sea salt contains important trace minerals, whereas they are mostly removed from table salt. Recommended amounts daily are 1/4 to 1/2 tsp in water twice a day…and some go a little higher, if needed.
Bob, a patient with excellent knowledge of low aldosterone, states: People with low aldosterone sufferer from "Salt Wasting", a medical term describing sodium leaving the body. When sodium is excreted it takes water with it, causing frequent urination and dehydration. The body will struggle to maintain a proper balance of sodium and potassium in the blood – and these levels often appear normal on blood tests. But within the cells of the body, improper balance of these minerals can lead to fatigue, and is the reason why the pupils will fluctuate when performing the "flashlight test". Persons with low levels of aldosterone crave salt. If they will take a minimum of 1/2 teaspoon of Sea Salt daily their symptoms improve. The "Salt Wasting" still occurs, but the symptoms of improper electrolyte balance will often improve, and they will feel more energy."
But….you have to be careful, as too muchsodium supplementation can drive aldosterone down even lower, and can increase your thirst all over again. A more important supplement can be potassium, which supports aldosterone levels, especially if potassium levels are low.
HOW DO I TEST FOR ALDOSTERONE?Testing for aldosterone will be either a 24 hour urine test or a blood test–the latter which is more highly recommended to pursue with your doctor. It may also be important to avoid all salt for 24 hours before the test, and to be moving around for two hours before you test. 8 am is a good time to do the test since aldosterone levels would be at their highest in the early morning. It's worthy to note that aldosterone levels can be doubled if you are pregnant, and are normally a little higher in children than in adults. For a complete picture, ask your doctor to include your renin for a complete picture, as well as sodium and potassium. See a testing facility without a prescription below.
You can also try a self-test–the pupil test, listed in Discovery Step Two on the Adrenal page. The blood pressure test from a supine position to standing can also point to your adrenals.
When lab testing, you are looking for 2 to 16 ng/dL if done laying down, and 5 to 41 ng/dL for upright. A good resource about results ishere. There can be some variations for different lab facilities. More in Chapter 5.
IMPORTANT NOTE FOR WOMEN: it is strongly recommended to test your aldosterone in the first week of your menstrual cycle and not later. Just as in pregnancy, higher progesterone levels, especially around mid-cycle and later, can drive your aldosterone falsely up, since aldosterone is made from progesterone.
WHAT MEDICATION DO I TAKE IF SEA SALT/POTASSIUM ISN'T ENOUGH TO TREAT MY LOW ALDOSTERONE? The treatment of choice is fludrocortisone acetate with the brand name Florinef, a very potent steroid with mineralocorticoid properties . Patients and their wise doctors have learned to start with a quarter pill (25 mcg or .025 mg) and raise by that amount every 5 to 7 days until they get to 100 mcg. (0.1 mg) rather than starting out on 100 mcg. Many will note good effects fairly quickly; others may need at least two weeks.
Florinef is a very powerful treatment, thus the reason to start low and work up in low amounts every week or so, patients have noted. Going up to 100 mcg is common, but you'll know if it's too much if your blood pressure goes up and potassium takes a serious dive. Check with your doctor for further information. It's also important to note that some patients who are already on HC (cortisol) may have to lower it to compensate for the glucocorticoid potency of Florinef. It's also recommended to take your Florinef with sea salt mixed in water.
Another method patients use to check on their Florinef use is the laying down/standing up blood pressure test. See Discovery Step Two, Test one, here. Bottom line, when using Florinef, keep track of your blood pressure, your pulse, and your electrolytes sodium and potassium.
Update: if you don't have hypopituitary or untreated diabetes, you can bring back BOTH your cortisol and aldosterone levels with the proper use of the T3CM and avoid the potential side effects of HC and Florinef. Read the link carefully.
WHY DO I NEED BOTH FLORINEF AND CORTEF SINCE BOTH ARE STEROIDS? If someone is hypopituitary or wasn't able to make the T3CM work well for them, and they know they have low aldosterone along with their low cortisol, why both steroid? Because Florinef (fludrocortisone) better imitates what Aldosterone does, and Cortef (hydrocortisone) better imitates what cortisol does.
Florinef has greater mineralcorticoid activity, just like Aldosterone does. To have mineralcorticoid activity means it controls electrolyte and water levels, mainly by promoting sodium retention in the kidney. (yours is low, thus the reason you urinate a lot, and lose salt because of that.).
Cortef has greater glucocorticoid activity, just like Cortisol does. To have glucocorticoid activity means it controls carbohydrate, fat and protein metabolism and is anti-inflammatory. It allows thyroid hormones to get to your cells.
So you can see that Cortef won't help you retain salt, just as Florinef won't help thyroid hormones get to your cells.
Go here to order your own tests.
Want to order your own labwork for aldosterone and renin, plus electrolytes?? STTM has created the right ones just for you to discuss with your doctor. Go here:https://sttm.mymedlab.com/
Need help interpreting your lab results? Go here:www.stopthethyroidmadness.com/lab-values/
SUCCESS STORIES:
TED: I started taking Florinef (100ug) two weeks ago, before knowing the dosing from Chris (i.e. not to start on 100ug). Never had a problem, and felt the difference the first day. All positive. Going off salt to take the aldosterone test isn't an option for me. I'd be in a coma long before the test date! I'm now on 40 mg Cortef, 120mg Armour, 100ug Florinef and feeling far better than I've felt in many years. I'm sure I'll stumble along the way as I increase the Armour, but I think I'm prepared for that. My constant "background" headaches have virtually disappeared……incredible!!!
MICHELLE: I have been on .1 mgs florinef for about 2 months now and what a difference. Before Florinef, I would drink and drink water and still was so puffy. And talk about being dehydrated! I would wake in the morning dying of thirst. I was constantly breathless, and my hearttrate was over 100 resting. Since being on Florinef, I notice increased energy towards the end of the day. I'm not so dehydrated and I handle heat alot better. I also don't feel so out of breath all the time. My pulse is now is 75-80. I don't need to take as much salt, since I think I get enough from my foods. I do notice if it is really hot out and I am sweating alot, I might do 1/4 tsp of sea salt and I am ok. For me I know I am taking too much sea salt when my legs cramp.
Have a Florinef success story? Send it via the STTM Contact below and we'll get your story up to inspire others. Keep it short like those above.
************
For more technical reading:
- Renal Tubular Effects of Hydrocortisone and Aldosterone in Normal Hydropenic Man: Comment on Sites of Action: http://www.jci.org/articles/view/105042
- Renal impairment resulting from hypothyroidism: http://ckj.oxfordjournals.org/content/1/6/440.full"
Tuesday, January 28, 2014
Describe Life after BLA
Nah. I don't feel like it. I don't want to write down all my happenings. I want to clearly explain everything but that takes time. I don't feel like explaining things today.
It has been 28 days since my BLA on 12/31/2014. The day of my surgery, I was given 300 mg of hydrocortisone intravenously. I was given 150 mg the next day. I have been tapering down since then. I left the hospital on a dose of 45 mg hydrocortisone at 7:30 am and 15 mg hydrocortisone at 3:00 pm. I added 0.05 mg fludrocortisone, a replacement for the hormone aldosterone, twice a day since I was post-op day 6. Every week or so, I decrease my hydrocortisone dose to something near 15/5. I am getting pretty close so that is good. My doctor will like that, because if I take more than my body needs, the extra hydrocortisone gives me Cushing's again. EEK! NO!
Last Sunday, I dropped my dose again from 20/5 to 17.5/5. I took the former dose for 7 or 8 days. Even that small of a drop takes the wind out of my sails. On Sunday, I woke at 7:30 am and was back asleep for a nap by 11:00 am. This, too, will pass.
I discovered that my dear friend Karen shared her post op BLA experience online and she provides clear explanation.
So today, I'll let Karen explain everything. I hope you feel well again soon.
http://m.caringbridge.org/visit/karenthames1/journal/entry/id/594801436/page/1/num/1
It has been 28 days since my BLA on 12/31/2014. The day of my surgery, I was given 300 mg of hydrocortisone intravenously. I was given 150 mg the next day. I have been tapering down since then. I left the hospital on a dose of 45 mg hydrocortisone at 7:30 am and 15 mg hydrocortisone at 3:00 pm. I added 0.05 mg fludrocortisone, a replacement for the hormone aldosterone, twice a day since I was post-op day 6. Every week or so, I decrease my hydrocortisone dose to something near 15/5. I am getting pretty close so that is good. My doctor will like that, because if I take more than my body needs, the extra hydrocortisone gives me Cushing's again. EEK! NO!
Last Sunday, I dropped my dose again from 20/5 to 17.5/5. I took the former dose for 7 or 8 days. Even that small of a drop takes the wind out of my sails. On Sunday, I woke at 7:30 am and was back asleep for a nap by 11:00 am. This, too, will pass.
I discovered that my dear friend Karen shared her post op BLA experience online and she provides clear explanation.
So today, I'll let Karen explain everything. I hope you feel well again soon.
http://m.caringbridge.org/visit/karenthames1/journal/entry/id/594801436/page/1/num/1
Friday, January 24, 2014
Change through Service

This quote clearly explains why I continue to work so hard to bring information to Cushies and change the medical world we must navigate. I can only hope that I can make an impact in this world.
A friend sent the quote below this week, and it immediately struck me in two ways:
1) Dr King's poignant reflection fifty years ago on what this country needed them and still needs now
2) the significance that such a statement holds for the Cushing's community of patients, advocacy community, and medical community of doctors and surgeons.
"One of the great liabilities of history is that all too many people fail to remain awake through great periods of social change. Every society has its protectors of status quo and its fraternities of the indifferent who are notorious for sleeping through revolutions. Today, our very survival depends on our ability to stay awake, to adjust to new ideas, to remain vigilant and to face the challenge of change."
- Martin Luther King, Jr.
Wednesday, January 15, 2014
If I Were an Owl...
... this would totally be me --
fighting for my
Cushing's diagnosis,
pituitary surgery date,
rediagnosis,
pituitary surgery date,
rediagnosis, and
adrenalectomy date.

Tuesday, January 14, 2014

Monday, January 13, 2014
My Favorite Poem
Cushies, stay strong in your fight for health and happiness.
Rudyard Kipling's If--
IF you can keep your head when all about you
Are losing theirs and blaming it on you,
If you can trust yourself when all men doubt you,
But make allowance for their doubting too;
If you can wait and not be tired by waiting,
Or being lied about, don't deal in lies,
Or being hated, don't give way to hating,
And yet don't look too good, nor talk too wise:
If you can dream - and not make dreams your master;
If you can think - and not make thoughts your aim;
If you can meet with Triumph and Disaster
And treat those two impostors just the same;
If you can bear to hear the truth you've spoken
Twisted by knaves to make a trap for fools,
Or watch the things you gave your life to, broken,
And stoop and build 'em up with worn-out tools:
If you can make one heap of all your winnings
And risk it on one turn of pitch-and-toss,
And lose, and start again at your beginnings
And never breathe a word about your loss;
If you can force your heart and nerve and sinew
To serve your turn long after they are gone,
And so hold on when there is nothing in you
Except the Will which says to them: 'Hold on!'
If you can talk with crowds and keep your virtue,
Or walk with Kings - nor lose the common touch,
If neither foes nor loving friends can hurt you,
If all men count with you, but none too much;
If you can fill the unforgiving minute
With sixty seconds' worth of distance run,
Yours is the Earth and everything that's in it.
Sunday, January 12, 2014
Pills to Live
My mama brought my meds to me in bed. After I took my 5 mg HC and 0.05 Florinef, I proudly announced, "Good. That'll keep me alive until the morning."
She didn't care for my joke.
Saturday, January 11, 2014
CUSHDAR
Cushdar is a word I made up 10 mins ago. Similar to radar and sonar, it's the keen sixth sense Cushies develop about their bodies and cortisol cycles that defy scientific or medical explanation. A Cushie always knows best.
In Search of the Perfect Siesta

Image courtesy of The Guardian.
I'm post op BLA day 11 and made it through day three at dose 25/5 (hydrocortisone 25 mg at 8 am, 5 mg at 3:30 pm). I dropped from 35/7.5 (12.5 mg is a little too big of a drop) because I had symptoms of high cortisol again: insomnia, 5 new pimples on my face, a small boil on my chest, and couldn't take a nap during the day for two days. Oh the misery! Haha Also, my mom pulled my husband aside and asked about my medication. She said I had been talking nonstop all day (no, really?!)
** A cortisol meter one day would be nice although I'm pretty impressed with my CUSHDAR. **
On 25/5, I am extremely fatigued by 1 pm and I have happily resumed napping for 2-3 hrs in the late pm. I have no other signs of AI. I am doing pretty well, but I wanted to post and explain my absence. My online and FB presence is spotty, and frankly what I see in the first 10 mins gets my attention for the hour I'm online. I wish everyone well and hope you are enjoying 2014. I love it. Best year yet.
PS. Did I already post about dropping dose and talking too much? Shoot. I don't even remember anymore.
Friday, January 10, 2014
Cushing's Support & Research Foundation
Cushing's Patient Education Day, 2014
The CSRF is holding a Cushing's Patient Education Day in Atlanta, GA, February 28 - March 1, 2014. You can register to attend through our website.
Click here for more information and to register
http://csrf.net/news-events/cushings-patient-education-day-2014/
Wednesday, January 8, 2014
Good news 7 days post op BLA
I wanted a quantitative way to track my progress post BLA. My mother, a fantastic seamstress, took my measurements in 12 different places on my body the night before my surgery. I will use this to monitor the impact of bilateral adrenalectomy and even assess whether I made the right decision for this irreversible treatment.
I also check in mentally and emotionally each day. I dug out and will restart my gratitude journal that Cushing's emotional imbalance kept me from filling. I feel happy and content. I'm not filled with rage and frustration, classic symptoms of high cortisol. I am grateful and filled with love. My mind is clear, and my heart is open. My body and my mind are no longer fighting. They are in harmony. I feel happy.
Cushing's never let me feel that way.
My body is no longer hanging on to fat because my cortisol is no longer high. Cortisol is the hormone that controls stress response. High cortisol tells your body to pack on fat to protect vital organs in event of bear mauling or being chased by a lion.
My abnormal adrenal glands (weighing 10 and 13 grams when normal is 4-6) were spewing cortisol out and flooding my body. My basement and whole house was under water, but even some doctors said no and blocked surgery.
On New Years Eve, I shut the valve of overflowing cortisol when I was brave enough to trust my body and agree to remove my adrenals. By taking steroid cortisol medication each day, I now take less than my body was making due to the tumors. I take 35 mg hydrocortisone at 7:30 am and 7.5 mg hydrocortisone at 3 pm to replace cortisol made in adrenals. I take 0.05 mg Florinef twice a day to replace the aldosterone hormone also made in the adrenals. I will take these pills, in varying doses, every day for the rest of my life.
Bilateral adrenalectomy is not the latest weight loss surgery. I am seeing results because tumors took over cortisol production and my body was flooded. Now my body is reacting--as it is built to do--by dropping weight it no longer needs.
Thank you for your love and support. It's an incredible ride.
-- Melissa
***Total inches lost***
7 days post op BLA
* measured by seamstress mama
** double checked many times for accuracy
** double checked many times for accuracy

Tuesday, January 7, 2014
Dr Friedman's Adrenal Gland Chapter

Guess who wrote the adrenal chapter of this very well-known and recognized medical textbook? Our very own Dr. Theodore Friedman!
"Students, residents, and instructors swear by Andreoli and Carpenter's Cecil Essentials of Medicine because it presents just the right amount of information, just the right way. Edited by the late Thomas E. Andreoli, MD as well as Ivor Benjamin, MD, Robert C. Griggs, MD, and Edward J. Wing, MD, it focuses on core principles and how they apply to patient care, covering everything you need to know to succeed on a medical rotation or residency. Masterful editing and a user-friendly full-color design make absorbing and retaining information as effortless as possible, and Student Consult online access offers convenient, flexible reference to the complete contents of the book plus additional clinical photos and radiologic images, videos demonstrating procedures, audio recordings of heart and lung sounds, and more."
This is a very comprehensive and informative read! Excellent job, Dr Friedman.
Monday, January 6, 2014
Patient vs. The Labs: Are You Ready?

>
> http://survivethejourney.blogspot.com/2012/04/day-16-of-cushings-awareness-challenge.html?m=1
Sunday, January 5, 2014
Bye Bye Adrenals, Hello New Friends

Adrenal glands, red in this image, are buried under all that human organ stuff in the abdomen.
I used to see BLAers, a term of endearment for those Cushies who have opted for surgical intervention with bilateral adrenalectomy, and watch them with awe and amazement, thinking they were BRAVE-- so brave to face uncertainty of Addison's because they knew, just knew, that shutting off the spiget of cortisol was the right thing to do. Taking that leap into the unknown is a very difficult thing to do, especially when the medical community and even family and friends warn you of the risks, lifelong changes, and irreversibility of the procedure.
Now that I have had my BLA, I *know* that we Cushie BLAers are brave, and that I am brave, too. This group of brave souls will save each other's lives over and over. We do so gladly. We reach out to one another for help and we hold on to one another in crisis. We are forever bonded by what we lack: adrenals.
Update
I was discharged on Friday on a dose of 45 mg hydrocortisone at 8 am and 15 mg hydrocortisone at 3 pm, plus Florinef 0.05 mg twice a day.
I have been napping a lot, and my mind is calm. My pain level is good--under control. I was hoping to feel this good a few weeks from now. I'm so HAPPY! My brain and body are no longer fighting each other. They now work together towards the common goal of health and wellness. Have a good Sunday, everyone!
- Melissa
Current dose is 40 and 15 hydrocortisone, or 40/15 for short.
I have been napping a lot, and my mind is calm. My pain level is good--under control. I was hoping to feel this good a few weeks from now. I'm so HAPPY! My brain and body are no longer fighting each other. They now work together towards the common goal of health and wellness. Have a good Sunday, everyone!
- Melissa
Current dose is 40 and 15 hydrocortisone, or 40/15 for short.
Wednesday, January 1, 2014

Tuesday, December 31, 2013
Update
2:21 pm pst - surgeon just visited. He and I are ready to go. He will grab a sandwich. I told him "No turkey!" I asked him to give me a local so I could live blog :D
Teaching Moments

Hi Olga!!
BLA on the way


Not many people here!
Very high tech hospital. QR codes on patient wrist band and very cool patient-in-surgery tracking system. My husband can look at a large screen in waiting room and know by the color where I am.
New Best Friend
I know I will make it through with my new best friend / favorite three words for this week:
~ patient-controlled dilaudid ~
~ patient-controlled dilaudid ~


Let's Get This Party Started
My surgery is scheduled for 1:00 pm on 12/31/2013. Call time is 10:30 am. I am the third surgery of the day. I am tired today after all the preparations and my pre-op appointment. I am happy not to be waking up so early but wishing I could go just to get on with this! I spent last night playing with my daughter and marveling in her. I love her, as she says, "infinity infinity one hundred thousand million.'

I made two word bubbles two years ago. The first one focused on the difficulties of life with Cushing's. This one focuses on new life once Cushing's is gone. Today, just in time for my BLA, I post this. It truly makes me smile knowing that these words mean so much to me as a sick person. With this surgery, I finally get my chance to get it all back and find my new places of joy. I can't wait to get back to traveling, running errands, visiting with my friends, walking around just to see what we could see. ROLLERBLADING! I really miss rollerblading. One day soon, I will be able to stand up on those inline skates and blade. I am grateful for all the opportunities for growth that lie before me.

I made two word bubbles two years ago. The first one focused on the difficulties of life with Cushing's. This one focuses on new life once Cushing's is gone. Today, just in time for my BLA, I post this. It truly makes me smile knowing that these words mean so much to me as a sick person. With this surgery, I finally get my chance to get it all back and find my new places of joy. I can't wait to get back to traveling, running errands, visiting with my friends, walking around just to see what we could see. ROLLERBLADING! I really miss rollerblading. One day soon, I will be able to stand up on those inline skates and blade. I am grateful for all the opportunities for growth that lie before me.
I want to share one of my favorite songs: Shania's Today is Your Day. I hope you like it as much as I do.
Happy New Year. It's gonna be the best one yet.
Melissa
Sunday, December 29, 2013
Goodbye Cushing's: Finally, I get my BLA
I am finally approved for my BLA in Los Angeles, CA for December 31, 2013. It's our wedding anniversary, so my husband said he would take me out to Beverly Hills for dinner and the place should be cool because we hear celebrities go there.
When I see the photos, I feel both sadness and hope. Sadness because of all the time I have lost to be my best self. Hopeful now that I can say goodbye to her and start a new life. Those two Melissas are gone. I will never be those people again. Hopeful because the new Melissa will be the MELISSA REMIX - the best combination of us all.
 I wanted to share this with all y'all here. I found blogging to be something that helps me make sense of what is happening to me, a place where I can PUT it and release it as I try to live every hour of my life. I am so pleased to hear that people relate to my experiences and they are rooting for me. I am rooting for you, too.
I wanted to share this with all y'all here. I found blogging to be something that helps me make sense of what is happening to me, a place where I can PUT it and release it as I try to live every hour of my life. I am so pleased to hear that people relate to my experiences and they are rooting for me. I am rooting for you, too.
I just got the final word from the surgeon on Saturday at noon that he will do my BLA on Tuesday.
There has been a lot of activity in the past two months. In November, I tested again and got the highest and most conclusive tests results confirming Cushing's once again. My Cushing's specialist cleared me for surgery. Surgeon set a surgery date of 12/17/13 and sent me to staff endocrinologists to confirm. First endocrinologist, a diabetes specialist, reviewed my case, said no, and blocked my surgery. After imploring the surgeon to help me, he scheduled an appointment with another endocrinologist. She was fascinated but perplexed by my case. I'm a medical curiosity! She invited another doctor in. I debated two endocrinologists at the same time for two hours. We spread all my photos, charts, lab results, MRI studies, and clinic notes across the table. They were misinformed on many aspects of the medical literature for Cyclical Cushing's but wouldn't listen to me. "Bilateral adrenalectomy is not reversible! You will be on medication the rest of your life! You will be miserable!" They blocked my surgery even though I had a doctor -- a NIH-trained physician who specializes in Cushing's and sees 1000 Cushing's patients in his practice -- who referred me to surgery. My surgery on December 17 was cancelled.
I left the hospital, dejected, uncertain, and suicidal. I know I am dying inside this broken body. My family circled the wagons and protected me. My mom flew in from out of state to help care for me, my husband, and daughter. She spent Christmas away from my father and family for the first time ever just to be with us. I continued to test per the deal I struck with the endocrinologists but I quickly tapped out. Three 24-UFCs with 17-ohcs, five midnight saliva cortisol tests, plus a low dose dexamethasone test really did me in. Test results showed even more high tests that point to hypercortisolemia: two high urine cortisols in 17-ohcs and two high MN cortisol salivas (2x and 3x upper limit of normal). I suppressed on dex test, as many cyclical Cushing'a patients do. My surgeon agreed to do the surgery again.
There has been a lot of activity in the past two months. In November, I tested again and got the highest and most conclusive tests results confirming Cushing's once again. My Cushing's specialist cleared me for surgery. Surgeon set a surgery date of 12/17/13 and sent me to staff endocrinologists to confirm. First endocrinologist, a diabetes specialist, reviewed my case, said no, and blocked my surgery. After imploring the surgeon to help me, he scheduled an appointment with another endocrinologist. She was fascinated but perplexed by my case. I'm a medical curiosity! She invited another doctor in. I debated two endocrinologists at the same time for two hours. We spread all my photos, charts, lab results, MRI studies, and clinic notes across the table. They were misinformed on many aspects of the medical literature for Cyclical Cushing's but wouldn't listen to me. "Bilateral adrenalectomy is not reversible! You will be on medication the rest of your life! You will be miserable!" They blocked my surgery even though I had a doctor -- a NIH-trained physician who specializes in Cushing's and sees 1000 Cushing's patients in his practice -- who referred me to surgery. My surgery on December 17 was cancelled.
I left the hospital, dejected, uncertain, and suicidal. I know I am dying inside this broken body. My family circled the wagons and protected me. My mom flew in from out of state to help care for me, my husband, and daughter. She spent Christmas away from my father and family for the first time ever just to be with us. I continued to test per the deal I struck with the endocrinologists but I quickly tapped out. Three 24-UFCs with 17-ohcs, five midnight saliva cortisol tests, plus a low dose dexamethasone test really did me in. Test results showed even more high tests that point to hypercortisolemia: two high urine cortisols in 17-ohcs and two high MN cortisol salivas (2x and 3x upper limit of normal). I suppressed on dex test, as many cyclical Cushing'a patients do. My surgeon agreed to do the surgery again.
I am comfortable in my decision and ready to move forward. Today, we will rally and get the house ready for my absence, and I'll started up a "feel good box" of things to keep me occupied during my time in the hospital.
When I see the photos, I feel both sadness and hope. Sadness because of all the time I have lost to be my best self. Hopeful now that I can say goodbye to her and start a new life. Those two Melissas are gone. I will never be those people again. Hopeful because the new Melissa will be the MELISSA REMIX - the best combination of us all.
 I wanted to share this with all y'all here. I found blogging to be something that helps me make sense of what is happening to me, a place where I can PUT it and release it as I try to live every hour of my life. I am so pleased to hear that people relate to my experiences and they are rooting for me. I am rooting for you, too.
I wanted to share this with all y'all here. I found blogging to be something that helps me make sense of what is happening to me, a place where I can PUT it and release it as I try to live every hour of my life. I am so pleased to hear that people relate to my experiences and they are rooting for me. I am rooting for you, too.
Well, Happy New Years Cushing's family!
May us all blossom in our new healthy state in 2014.
Melissa
Tuesday, December 17, 2013
Patient Information for Laparoscopic Adrenal Gland Removal (Adrenalectomy) from SAGES
I thought this was a good read. It includes things to do pre-op that I haven't seen written down. Most of these, though, don't always discuss the removal of both adrenal glands, which is really a different matter in terms of replacing hormones, recovery time, and after care.
Society of American Gastrointestinal and Endoscopic Surgeons
http://www.sages.org/publications/patient-information/patient-information-for-laparoscopic-adrenal-gland-removal-adrenalectomy-from-sages/
Society of American Gastrointestinal and Endoscopic Surgeons
http://www.sages.org/publications/patient-information/patient-information-for-laparoscopic-adrenal-gland-removal-adrenalectomy-from-sages/
Sunday, December 8, 2013
Inflammation: Why You STILL Have Low Thyroid Symptoms
I can truly appreciate this video of a doctor explaining how a patient with hypothyroid symptoms show normal lab results, stump doctors, and get passed around but never treated. This has happened to me! I, too, have inflammation, and everyone including the PCP, chiropractor, acupuncturist, endocrinologist, rheumatologist, and psychiatrist have all taken note of my edema, or swelling. My massage therapist ALWAYS says by body is inflamed.
So, this doctor seems to understand the runaround that patients get, explains why we get the runaround, and offers advice about how to solve the inflammation "problem." He has a series of YouTube videos. I'll make my way through them eventually. - Melissa
Hidden Cause #20 Why You STILL Have Low Thyroid Symptoms - Inflammation Blocks T3 Receptor
http://youtu.be/ljRWZ9gCxws
Friday, December 6, 2013
Life Lines: My Cushie Friends
In life's game of Who Wants to be a Healthy Patient, my phone-a-friend lifeline will be a Cushie friend over any endocrinologist, any day of the week and twice on Sunday.

Thursday, December 5, 2013
Cushing's, Cortisol and Receptors
More research from the Dutch and Germans. I have no idea what this means! My Cushie brain can not piece together this new information.
I have never heard the term "normocortisolism."
Preoperative Normalization of Cortisol Levels in Cushing's Disease After Medical Treatment: Consequences for Somatostatin and Dopamine Receptor Subtype Expression and In Vitro Response to Somatostatin Analogs and Dopamine Agonists
http://m.jcem.endojournals.org/content/98/12/E1880.abstract
Support your Loved One with Chronic Pain

Pete Beisner knows a lot about supporting a partner in chronic pain. Here, he shares insights on how to take care of the person you love. He authored this poignant and impressive read, entitled 23 Tips For Men on Supporting a Partner with Chronic Pain.
As a person who suffers from chronic pain, I am happy to know that a way to help has been so clearly defined. Some days, the pain is so bad, I just don't know how I can do it or what I need to make it go away. This list offers a sort of menu of options, things that someone can do without me having to tell them first.
Thank you, Pete and NAIDW for this wonderful article. ~ Melissa
Solu-Cortef on the Ambulances
Print this flyer and give to your EMS team
Non-Green States => Preventable Deaths

CARES Foundation is another non-profit organization that is working to educate EMS professionals while getting Solu-Cortef on every ambulance. Their members face congenital adrenal hyperplasia and need the hydrocortisone dose via Solu-Cortef, too. They keep track of legislative status by state and advocates for us to make the change happen in our town and state.
We have a long way to go before these states are all green. So, let's all get started and help our friends. -M
Hey EMS Professionals: Study Up
Kudos to the Massachusetts Department of Public Health for developing and sharing this presentation.
"This presentation is intended for EMTs of all certification levels. We recommend that you review the slides from start to finish, however hyperlinks are provided in the table of contents for fast reference. Certain slides have additional information in the ‘notes’ section. This presentation was created by MA EMS for Children using materials and intellectual content provided by sources and individuals cited in the “Resources” section. "
"This presentation is intended for EMTs of all certification levels. We recommend that you review the slides from start to finish, however hyperlinks are provided in the table of contents for fast reference. Certain slides have additional information in the ‘notes’ section. This presentation was created by MA EMS for Children using materials and intellectual content provided by sources and individuals cited in the “Resources” section. "
Southern Nevada Health District's Office of Emergency Medical Services
& Trauma System gets it right.
& Trauma System gets it right.
Share this with your local EMS team.
Wednesday, December 4, 2013
RIP Sarah: Another Senseless Cushie Death
 |
| Sarah Thomas, 30, died six hours after EMS refused to take her to the hospital oradminister her the life-saving Solu-Cortef injection. |
I send my most sincere condolences to Sarah's friends and family.
I am so rattled. This is unjust. It's so avoidable!
A simple injection of Solu-Cortef could have saved Sarah. It costs less than $10.
Taking Sarah to the hospital could have saved her.
Something must be done to stop the medical profession's ignorance about adrenal insufficiency and cavalier know-it-all attitude.
We must be able to count on someone to help us. How can we rest easy each day, wondering who will listen, who will believe us?
Please support the group, Adrenal Insufficiency United, whose goals are to educate EMS personnel and ensure that Solu-Cortef is carried on every ambulance in the US. Purchase one of their emergency kits and give a CD to the fire stations in your area.
You will save others as you work to save yourself. - Melissa
*****************
You will save others as you work to save yourself. - Melissa
*****************
Incompetent paramedics told dying woman: ' You just have a tummy bug'
Woman would have survived if she was taken to hospital and given a simple injection
Two paramedics have been struck off for blundering over the tragic death of a dental nurse after telling her: "You just have a tummy bug."
Sarah Thomas, 30, died at home because her symptoms were not taken seriously by the two "incompetent" ambulancemen who refused to take her to hospital.
Paramedic David Glover told her she just had the stomach bug – even though she was barely conscious and struggling to breathe.
Ms Thomas would have survived if she was taken to hospital and given a simple injection. But she died six hours later.
A disciplinary hearing was told Glover and colleague Michael Davies then tried to cover up their mistake by fabricating her clinical record.
The pair were banned from working as paramedics by a disciplinary panel of the Health and Care Professions Council.
Panel chair Ian Crookall said: "The public would be appalled at the lack of competence.
"The facts of the case would undermine public confidence in the profession in the eyes of any member of the public who was aware of the circumstances.
"When there is a case of proven dishonesty it is necessary to uphold regulatory standards by demonstrating that such behaviour is not acceptable."
Sarah was visited at her home in Port Talbot, South Wales, by the two paramedics following a 999 call.
A Health and Care Professions Council hearing was told how Glover failed check her vital signs including pulse, breathing and blood oxygenation.
Ms Thomas had diabetes and her pituitary gland had been removed after surgery for a brain tumour. (Blogger note: Sarah had Cushing's and secondary adrenal insufficiency after pituitary surgery).
But the hearing in Cardiff was told that Glover failed to ask suitable questions about her medical history.
He told her: "You just have a stomach bug. You are better off here Sarah, this is the best place for you".
But Ms Thomas died just six hours later of adrenal insufficiency – when her body stopped producing the necessary steroid hormones. (Blogger emphasis).
Glover and Davies, who were working for the Welsh Ambulance Service NHS Trust, then "colluded to fabricate a patient record".
The pair added information they got later from another paramedic in an attempt to cover up their failures.
Mr Crookall added: "The panel was of the view that the established failure to conduct a proper assessment.
"The subsequent dishonest fabrication and collusion are very serious, representing a disregard for fundamental and core duties.
"It had the potential of causing very significant degree of harm – including death."
**************
I only have two words: NO SHIT (Blogger emphasis).
**************
I only have two words: NO SHIT (Blogger emphasis).
Subscribe to:
Posts (Atom)